Well, not for the moment, at least. But watch out.
I didn't have time to go for my camera before this moment disappeared, so I settled for this with my phone.
Well, not for the moment, at least. But watch out.
I didn't have time to go for my camera before this moment disappeared, so I settled for this with my phone.
Paternity leave, Day number I'm not sure anymore. It's not such a lovely day today as it was the last two (70s-80s, sunny, mountains out...), but still the outside was inviting, so after two cups of strong drip coffee I strapped Elliott to my chest, put a leash on Yagi, and headed out for a walk around Beacon Hill. Our destination was, bien sur, Galaxie, but the route was to be improvised. I've not yet walked through that neighborhood, and was quite pleased with the sights. There are great views of the mountains and across the valley to the Mount Baker neighborhood. The housing in dense and old, mostly. Lots of old craftsman homes from the 1920s, many are well-maintained, but there are a few that need some love. There are also a bunch that qualify as tear-downs.
We wound our way up the hill, following interesting sights and quiet streets on our way to the coffee shop. I spoke with my mom for a while while we walked, and she told me of her afternoon yesterday with Zoë, who is visiting St. Louis with Brooke this week.
 Jerome Groopman has been all over NPR the last few days giving interviews about his new book, How Doctors Think. This morning he landed a seven-minute session on Morning Edition, and recently spoke at length with Terry Gross on Fresh Air. The book sounds like a well-constructed inquiry into the algorithmic processes of doctor think. How do physicians make sense of patients' stories and arrive at a diagnosis?
Jerome Groopman has been all over NPR the last few days giving interviews about his new book, How Doctors Think. This morning he landed a seven-minute session on Morning Edition, and recently spoke at length with Terry Gross on Fresh Air. The book sounds like a well-constructed inquiry into the algorithmic processes of doctor think. How do physicians make sense of patients' stories and arrive at a diagnosis?An anchoring mistake? Sounds like what my people call early closure, a very common"Usually doctors are right, but conservatively about 15 percent of all people are misdiagnosed. Some experts think it's as high as 20 to 25 percent. And in half of those cases, there is serious injury or even death to the patient."
Why do you think that doctors would be wrong that often?
Well, you know, it's very hard to be a doctor. We're working under tremendous time pressure, especially in the current medical system. But the reasons we are wrong are not related to technical mistakes, like someone putting the wrong name on an X-ray or mixing up a blood specimen in the lab. Nor is it really ignorance about what the actual disease is. We make misdiagnoses because we make errors in thinking.
We use shortcuts. Most doctors, within the first 18 seconds of seeing a patient, will interrupt him telling his story and also generate an idea in his mind [of] what's wrong. And too often, we make what's called an anchoring mistake — we fix on that snap judgment.
 problem. Making big differentials is hard, and many things influence how quickly we decide we know the diagnosis. Often, it just seems to fit...mostly...more than other stuff. But is our list comprehensive? Did we consider only common diagnoses? Is is time to trot out the rare, eponymous syndromes we memorized in med school but have never seen? Deciding early to attach a diagnosis to a symptom feels good, especially when there are other patients with symptoms waiting to be seen.
problem. Making big differentials is hard, and many things influence how quickly we decide we know the diagnosis. Often, it just seems to fit...mostly...more than other stuff. But is our list comprehensive? Did we consider only common diagnoses? Is is time to trot out the rare, eponymous syndromes we memorized in med school but have never seen? Deciding early to attach a diagnosis to a symptom feels good, especially when there are other patients with symptoms waiting to be seen."The Match" -- a high-anxiety cap to the end of a grueling four-year medical education -- will determine their professional futures, not just where they will live for the next three to seven years, but what specialty they will pursue.Well, that all sounds quite difficult, doesn't it? True, medical training isn't easy, but it's not Darfur. There's a language tossed around in the press that creates this mystique of systematic torture by drill-sergeant faculty.
There's a buzz going on, but the excitement has the tamped-down quality of people who have learned to manage anxiety to survive the rigors of clinical rotations, being called out for not knowing answers during rounds and monster exams.
There is recognition, too, that as hard as medical school was, residencies, renowned for their brutal on-call schedules, can be even harder.

 eventually onto the I-405 HOV lane, which moved at about 60mph while the other three lanes literally sat still. Traffic was miserable all over due to accidents and a big police foo-faa over a stolen car.
eventually onto the I-405 HOV lane, which moved at about 60mph while the other three lanes literally sat still. Traffic was miserable all over due to accidents and a big police foo-faa over a stolen car. I'm off work this week. It's good. We thought about going away for a few days, renting a cottage on Whidbey Island or Hood Canal. That would be good fun, if it weren't for Zoë and Elliott and their dueling sleep schedules...well, their awake schedules, I should say. It's bloody exhausting. Weekends turn out to be pretty hard, and three days in a cottage, even in a lovely setting and even with a hot tub, would have been less like a vacation than like work. The alternative was to stay in Seattle, send Zoë off to day care in the morning, and enjoy life with one very portable infant. We can take naps, write, go for walks, get massages, all thanks to the happy two-parent-to-one-child ratio we used to think was so hard. Yesterday we called Sam to babysit for the afternoon, then headed out for lunch at High Spot and a walk. No nap.
I'm off work this week. It's good. We thought about going away for a few days, renting a cottage on Whidbey Island or Hood Canal. That would be good fun, if it weren't for Zoë and Elliott and their dueling sleep schedules...well, their awake schedules, I should say. It's bloody exhausting. Weekends turn out to be pretty hard, and three days in a cottage, even in a lovely setting and even with a hot tub, would have been less like a vacation than like work. The alternative was to stay in Seattle, send Zoë off to day care in the morning, and enjoy life with one very portable infant. We can take naps, write, go for walks, get massages, all thanks to the happy two-parent-to-one-child ratio we used to think was so hard. Yesterday we called Sam to babysit for the afternoon, then headed out for lunch at High Spot and a walk. No nap. might post if Brooke can get over thinking our children will end up like the Star Wars kid or that poor Numa Numa Dance fellow. I don't see it happening with the bath video, but maybe with Zoë's "Shake Your Booty" song.
might post if Brooke can get over thinking our children will end up like the Star Wars kid or that poor Numa Numa Dance fellow. I don't see it happening with the bath video, but maybe with Zoë's "Shake Your Booty" song. usually following publication of research or polls. I'm interested in what contributes to satisfaction in the patient-doctor relationship, though I'm not convinced that we need to be satisfied to have our needs met. Or, put another way, offering the best and safest medical care may not always satisfy my patients--or me. There is a lot of research about satisfaction, but no clear evidence that satisfaction matters. It is assumed to be its own valid outcome, though it is hard to measure reliably. There are a couple of fun satisfaction items that have landed in my Google Reader recently.
usually following publication of research or polls. I'm interested in what contributes to satisfaction in the patient-doctor relationship, though I'm not convinced that we need to be satisfied to have our needs met. Or, put another way, offering the best and safest medical care may not always satisfy my patients--or me. There is a lot of research about satisfaction, but no clear evidence that satisfaction matters. It is assumed to be its own valid outcome, though it is hard to measure reliably. There are a couple of fun satisfaction items that have landed in my Google Reader recently. And what about satisfaction? "Patient satisfaction and trust remained high, regardless of whether expectations were met." So what can I learn from this study? Should I worry about what patients expect? If expectations aren't related to satisfaction, well then what is? And does satisfaction matter? I know plenty of people who aren't satisfied with their doctors, but they keep going.
And what about satisfaction? "Patient satisfaction and trust remained high, regardless of whether expectations were met." So what can I learn from this study? Should I worry about what patients expect? If expectations aren't related to satisfaction, well then what is? And does satisfaction matter? I know plenty of people who aren't satisfied with their doctors, but they keep going.Already this seems more useful than the Annals piece, as they ask whether patient health actually improved. I'm also happy CR asked about respect, but shocked that so few doctors listen to and respect their patients. CR presents this under the good news header!
The bad news for physicians: The majority of patients said their doctors never talked to them about the cost of treatments and tests.
I hate talking money with patients, and frankly feel ill-equipped to do it. I know tons about tests and treatments, but very little about what they cost. My ePocrates handheld reference gives me some info, but I can't predict what insurance will cover and at what rate. I saw a patient in clinic one day with chest pain. It wasn't his heart, but when I shared with him some chest pain (i.e. heart attack) warning signs that should prompt him to call 911, he began to quiz me on on the costs of ambulance transport and emergency care. I had no idea what to tell him, and felt bad about it. I know money matters, but I just don't have the answers.
In addition, patients had these complaints:
• 74 percent said their physicians had not asked about emotional stress.
• 24 percent said their physicians made them wait 30 minutes or more.
• 19 percent said they couldn't get an appointment within less than a week.
 I cannot believe that there are still non-surgeon physicians who don't ask about stress. The second two complaints above are systems issues, and inexcusable. I think making patients wait around to see a doctor demonstrates a real lack of respect for the value of their time. Patients don't have all day to hang out in clinics, waiting to be seen. Also, having to wait a week when you're sick or when your kid is sick and you're worried is just plain wrong. Who wouldn't go to the ER under those circumstances? Same day or next day access isn't that hard to provide; we should be doing it.
I cannot believe that there are still non-surgeon physicians who don't ask about stress. The second two complaints above are systems issues, and inexcusable. I think making patients wait around to see a doctor demonstrates a real lack of respect for the value of their time. Patients don't have all day to hang out in clinics, waiting to be seen. Also, having to wait a week when you're sick or when your kid is sick and you're worried is just plain wrong. Who wouldn't go to the ER under those circumstances? Same day or next day access isn't that hard to provide; we should be doing it.
• 41 percent said that patients wait too long before making an appointment.
Or are they just waiting for their appointment?
• 32 percent said patients are too reluctant to talk about their symptoms.
Except emotional stress, which we don't want to talk about.
• 31 percent said patients request unnecessary tests.
Bloody internet.
• 28 percent said patients request unnecessary prescriptions.
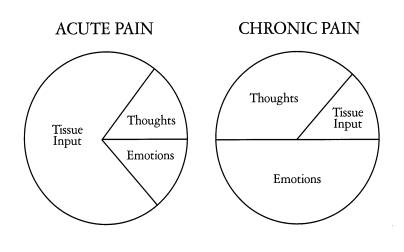
Bloody advertising. In this case, I refer back to the Annals paper, which reminds us that it is important to negotiate with patients. We shouldn't offer wasteful or harmful interventions to patients, even if they want them. We should offer alternatives that address patient concerns and hopes. Recently, my residency program has been working on how we help patients with pain. Honestly, some of this comes from the great frustration the doctors and staff at our three clinics feel with "pain patients." It feels like patients with chronic pain take up a lot of our time and energy, and we end up not helping them very much--they still have pain. Stuck in our doctor brains is the notion that if something is wrong, we should be able to fix it, or at least help patients fix it. So when things don't get better--the pain is the same or worse--over months of treatment, we get frustrated, and so do our patients.
Recently, my residency program has been working on how we help patients with pain. Honestly, some of this comes from the great frustration the doctors and staff at our three clinics feel with "pain patients." It feels like patients with chronic pain take up a lot of our time and energy, and we end up not helping them very much--they still have pain. Stuck in our doctor brains is the notion that if something is wrong, we should be able to fix it, or at least help patients fix it. So when things don't get better--the pain is the same or worse--over months of treatment, we get frustrated, and so do our patients.
 A couple of weeks ago I put together a five page "Menu of Treatments for Low-Back Pain" for one of my patients. I had hoped to use some chronic disease management techniques to create a plan with her that would be as transparent as possible. I created the menu from the collected works of the Cochrane Back Group and offered it to her as a way to start us both thinking about how to help her to a tolerable level of pain. The menu concept is popular in managing chronic diseases like diabetes and hypertension that require patients to change behaviors. It gives people options and lets them choose what they think they can do. It is important to build the menu around goals--another chronic care pillar--and so we spent some time discussing what she hoped to accomplish regarding her pain. I thought it went well.
A couple of weeks ago I put together a five page "Menu of Treatments for Low-Back Pain" for one of my patients. I had hoped to use some chronic disease management techniques to create a plan with her that would be as transparent as possible. I created the menu from the collected works of the Cochrane Back Group and offered it to her as a way to start us both thinking about how to help her to a tolerable level of pain. The menu concept is popular in managing chronic diseases like diabetes and hypertension that require patients to change behaviors. It gives people options and lets them choose what they think they can do. It is important to build the menu around goals--another chronic care pillar--and so we spent some time discussing what she hoped to accomplish regarding her pain. I thought it went well.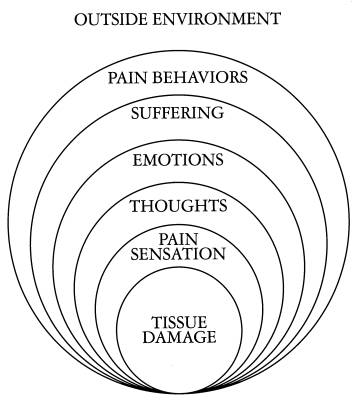
 Inspired by a recent post by Bus Chick, I snapped this (phone camera) shot a few minutes ago near my house in the Rainier Valley. I saw lots of tiny blooms on my walk to and from Dahlia Spa. Seeing new blooms in Seattle means that it must be February. The days are finally getting a little longer, and soon we'll all be making vitamin D again. It turns out to be just about the nicest day in recent memory here: thin cloud-cover and a mild 57-degrees as I write.
Inspired by a recent post by Bus Chick, I snapped this (phone camera) shot a few minutes ago near my house in the Rainier Valley. I saw lots of tiny blooms on my walk to and from Dahlia Spa. Seeing new blooms in Seattle means that it must be February. The days are finally getting a little longer, and soon we'll all be making vitamin D again. It turns out to be just about the nicest day in recent memory here: thin cloud-cover and a mild 57-degrees as I write.